
Roughly 1 in 8 women will be diagnosed with breast cancer in their lifetime. The survival rate for Stage I detection is over 99%. For Stage IV, it drops below 30%.
That gap comes down to when and how accurately the tumor was found.
The imaging tools have existed for decades. Mammograms, MRI, ultrasound, all widely used. The limitation is rarely whether a tumor shows up on a scan. It is whether the boundary of that tumor is identified precisely enough to act on. A suspicious region that is detected but poorly localized still leaves a clinician without the information needed to stage accurately, plan a biopsy, or track change over time.
AI segmentation is built to close that gap. It sharpens the precision of what gets handed to the radiologist.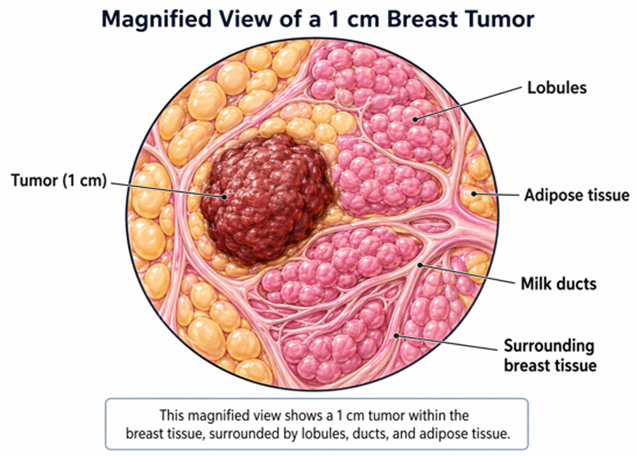
Fig: Cellular abnormalities, tumor formation, imaging representation, Magnified View of 1 cm Breast Tumor
This article examines how deep learning models perform AI breast cancer segmentation on ultrasound images, what evaluation metrics actually tell clinical teams about model readiness, and where current models still fall short.
Detection and Localization Are Not the Same Problem
Most people, when they hear ‘AI cancer detection,’ picture a model that flags suspicious scans. That is classification: the model looks at an image and outputs a probability that cancer is present.
AI segmentation is a harder and more clinically useful task. A segmentation model produces an output for every pixel in the image. Each pixel gets a label: tumor or healthy tissue. The result is a precise mask overlaid on the original scan, tracing the exact boundary of the lesion.
Tumor size, margin characteristics and spatial relationship to surrounding structures all feed into staging and treatment decisions. A system that identifies cancer without localizing it precisely answers only part of the diagnostic question.
This is why AI for breast cancer diagnosis increasingly relies on segmentation workflows rather than image-level classification alone.

Fig: Illustration of the end-to-end segmentation work-flow: input scan → model inference → predicted mask overlay
Ground Truth vs. Predicted Mask
The effectiveness of deep learning medical image segmentation depends on how closely the model output matches expert annotations.
The ground truth mask is the reference annotation, drawn by a radiologist or trained clinical annotator. The predicted mask is what the AI model produces after analyzing the image. The training process minimizes the gap between the two.
Expert disagreement can occur at lesion boundaries, which is why the most rigorous studies use multiple annotators and report the range of agreement rather than treating any single mask as final.
This matters because AI cancer detection systems are being evaluated against standards that even human experts do not interpret identically in every case.
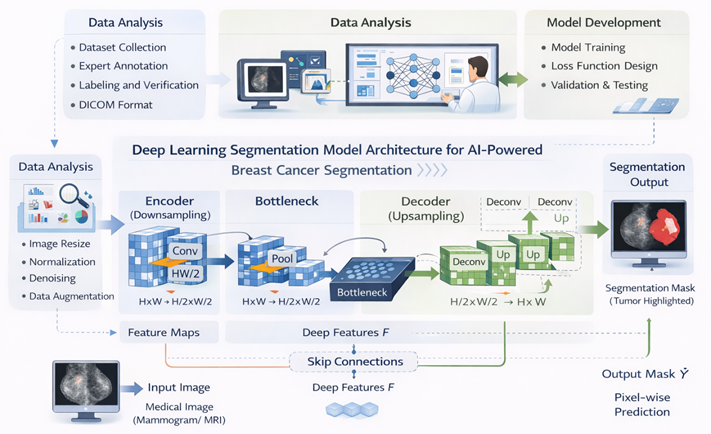
Fig: Deep Learning Segmentation Model Architecture for AI-Powered Breast Cancer Segmentation

Fig: Visually comparing original image → ground truth mask → predicted mask is the standard method for communicating segmentation quality to clinical stakeholders
How AI Segmentation Model is Built and What it Learns
The architecture used most widely for deep learning medical image segmentation is U-Net. It is designed specifically for tasks where precise spatial boundaries matter and labeled training data is limited.
U-Net works in two stages.
-
The first stage compresses the image progressively, extracting patterns at increasing levels of abstraction: edges, textures, shapes and structural relationships.
-
The second stage reverses that process, using the learned patterns to reconstruct a full-resolution output mask.
Skip connections between the two stages preserve fine spatial detail that would otherwise be lost in compression.
At every pixel, the model outputs a probability: how likely is it that this pixel belongs to the tumor? A threshold of 0.5 converts those probabilities into a binary mask.
Attention mechanisms, added on top of the base architecture, allow the model to weigh its focus toward regions most likely to contain tumor. Spatial enhancement modules improve sensitivity around lesion boundaries, which are often the most clinically important regions.
Why Ultrasound Makes AI Segmentation Harder
Ultrasound plays an important role in AI breast cancer imaging because it is widely available, radiation-free and effective for dense breast tissue. But it produces images that are genuinely difficult to segment automatically.
Speckle noise is inherent to how ultrasound works. Contrast between the tumor and surrounding tissue is often low. Artifacts can appear that mimic real anatomy. Malignant lesions frequently have indistinct, irregular edges, and experienced radiologists themselves sometimes disagree on those boundaries when annotating independently.
Standard image segmentation architectures designed for high-contrast photographs do not transfer cleanly to this environment. The core challenge is preserving fine boundary detail while capturing enough surrounding context to distinguish a tumor from normal tissue variation.
This is one reason AI detects cancer more reliably when segmentation models are trained specifically for medical imaging workflows rather than adapted directly from general-purpose computer vision systems.
Dataset Evaluation and Model Performance
The segmentation framework was evaluated using a publicly available dataset containing 780 annotated breast ultrasound images across normal, benign and malignant categories.
The architecture combined U-Net, attention mechanisms and spatial enhancement modules.
The results included:
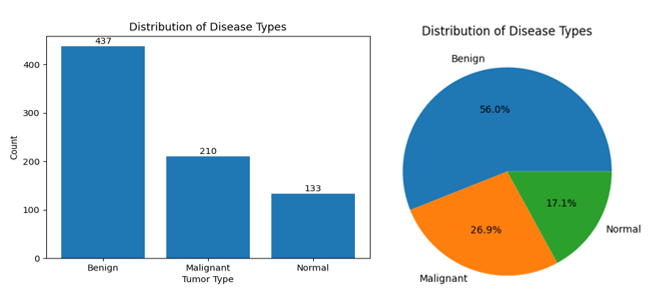
Fig: Proportional breakdown of the three ultrasound categories
- Test accuracy: 85.47%. The model correctly classified tumor versus non-tumor pixels on images it had not seen during training.
- Validation IoU: 0.4993. Approximately half of every predicted tumor region overlapped precisely with the expert annotation.
- Test IoU: 0.4974. Consistent with validation, confirming the model generalized rather than overfitting to training data.
An IoU of approximately 0.50 is a genuine baseline result for breast ultrasound segmentation. It demonstrates that the model has learned meaningful tumor structure and that the attention and spatial enhancement modules are contributing real improvement over standard CNN baselines, particularly on malignant cases where boundary ambiguity is highest.
It also shows where the next phase of work sits: improving boundary precision on lesions with irregular or diffuse edges. The consistency between validation and test performance is the more important signal here.
A model that holds its IoU across unseen data is behaving predictably, and that is the baseline requirement before any clinical pipeline consideration can begin.
Proof Point from a Breast Ultrasound Segmentation Use Case
A healthcare research team required a reproducible approach for localizing breast tumors in ultrasound scans where manual interpretation varied across observers. The team implemented a U-Net encoder-decoder architecture supported by attention mechanisms and spatial enhancement modules.
The system was trained on 780 annotated breast ultrasound images spanning normal, benign, and malignant categories.
Performance evaluation used Dice Similarity Coefficient (DSC) and Intersection over Union (IoU).
Outcomes
- Test accuracy reached 85.47% on unseen image data
- Validation accuracy peaked at 93.33% during training
- Validation IoU reached 0.4993

Fig: Comparison of breast ultrasound images with predicted segmentation masks and actual ground truth masks
The consistency between validation and test performance demonstrated that the model generalized effectively instead of memorizing training samples.
What Healthcare Teams Should Focus on Nex
Breast cancer segmentation is still evolving, but the gap between predicted masks and expert annotations continues to narrow.
The conversation is also changing.
The focus is no longer limited to whether AI models can segment accurately under controlled conditions. Healthcare organizations now need to evaluate how reliably those models perform across:
- Diverse patient populations
- Different imaging devices
- Multiple clinical environments
- Real-world diagnostic workflows
Models trained on isolated datasets must be validated against broader imaging conditions. Edge cases must remain visible during evaluation. Infrastructure such as annotation workflows, monitoring systems and data pipelines must meet clinical reliability standards from the beginning.
Organizations investing in those foundations today will be better positioned to scale future diagnostic AI initiatives responsibly.
Conclusion
AI segmentation is improving the precision and consistency of breast tumor localization in medical imaging workflows.
The progress is especially important for AI cancer detection systems where accurate localization directly influences diagnosis, staging and treatment planning.
The next phase of adoption will depend less on proving that models work in research settings and more on operationalizing them reliably across healthcare systems.
At Accion Labs, teams work with healthcare and life sciences organizations to build scalable AI and data engineering foundations for diagnostic workflows, medical imaging systems and clinical AI platforms. This includes support for production-ready machine learning pipelines, imaging data integration and AI model operationalization aligned with healthcare delivery environments.
Frequently Asked Questions
1. What is AI segmentation in breast detection?
AI segmentation in breast cancer detection is the process of training a deep learning model to identify and trace the exact boundary of a tumor in a medical image, pixel by pixel. A classification model tells you whether cancer is present. A segmentation model tells you where the tumor is, how large it is, and how its edges relate to surrounding tissue. That information directly supports staging, biopsy planning and treatment decisions.
2. How accurate is AI in detecting breast cancer from ultrasound images?
Accuracy depends on the model architecture and dataset. In a U-Net based framework evaluated on 780 annotated breast ultrasound images, test accuracy reached 85.47% and the Intersection over Union (IoU) score was approximately 0.50. This means the model's predicted tumor boundary overlapped with the radiologist's annotation about half the time. It is a meaningful baseline, but most clinical teams require higher IoU scores and multi-site validation before deploying a segmentation model in a live diagnostic workflow.
3. What is the difference between AI cancer detection and AI segmentation?
AI cancer detection typically refers to classification: the model reviews a scan and outputs a probability that cancer is present. AI segmentation goes further. It maps every pixel in the image as either tumor tissue or healthy tissue, producing a mask that traces the lesion boundary. Segmentation requires more precisely annotated training data and is evaluated using spatial overlap metrics like Dice Similarity Coefficient and IoU rather than standard classification accuracy.